
Acromegaly in a Patient with Papillary Thyroid Cancer
Case report
Additional Files
Published
How to Cite
Issue
Section
License
Copyright (c) 2020 Noemí Lourdes Bautista Litardo, Romina Moncayo R., Caroll Bombón P, Karen Ojeda D; EDITOR: Katherine García Matamoros

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.




DOI:
https://doi.org/10.33821/485Keywords:
Acromegaly, Thyroid Cancer, Papillary, Thyroid gland, Pituitary neoplasms, Thyroid neoplasms, Case reportsAbstract
Introduction: Thyroid cancer is the most frequent endocrine neoplasia and Papillary thyroid carcinoma represents 80% of cases. On the other hand, acromegaly is a poorly diagnosed disorder with an estimated annual incidence of 4 cases per million people. We present a case in which the two entities occur at the same time in a patient and the discussion of the possible biochemical link.
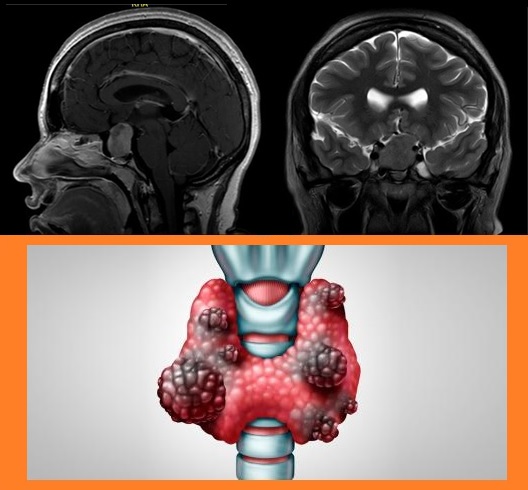
Clinical case: 23-year-old woman, with a 3 cm stone nodular mass in the upper pole of the right thyroid lobe; submitted to radical thyroidectomy and bilateral cervical lymphadenectomy, histopathological report of papillary carcinoma. It evolves with visual changes in the left eye, headache, 1-year amenorrhea, negative galactorrhea, morpho-anatomical characteristics of acromegaly, left homonymous hemianopia campimetry. T2 hyperintense seal and suprasellar lesion brain MRI in relation to pituitary macroadenoma. Biochemicals: Prolactin 131.20, GH 2.7, ACTH 18.5, IGF1 434, IGFBP 35.8, TTOG for reported GH: GH 0 min: 10.7, GH 30 min: 9.24, GH 60 min: 7.9.
Evolution: The patient underwent partial endoscopic transsphenoidal hypophysectomy. In treatment with cabergoline 0.5 mg twice weekly, levothyroxine 225 mcg day and octreotide 20 mg monthly.
Conclusion: It is concluded that, being acromegaly a rare disease, it is associated with thyroid cancer, involving possible mutations in the ? subunit of the G protein.