Fibrous bone dysplasia: A case report
Article / Artículo
https://doi.org/10.33821/730
Date received: 23/12/2023
Date accepted: 29/3/2024
1. Introduction
Fibrous bone dysplasia is a rare, benign, and congenital pathology that affects the
skeletal development of the human body by altering the normal composition of the bone
[1]. It has a global prevalence of 1/100 000 inhabitants and comprises 5% of all primary
bone tumors [2]. Although its etiology is not clear, post-zygomatic mutations of the GNAS gene,
located on chromosome 20, have been identified. They lead to the stimulation of adenylyl
cyclase and subsequent overproduction of cyclic adenosine monophosphate with uncontrolled
cell proliferation and inadequate differentiation [1,3]. Its clinical spectrum is broad, it could be accompanied by dermatological or endocrinological
disorders. The diagnosis is made through clinical history, radiological studies depending
on the affected bone, and histopathological investigation. Management focuses on observation,
pharmacological use with bisphosphonates and surgical treatment [4,5]. There are very few reports in national medical literature on this benign pathology,
which is why its scientific dissemination is considered essential.
2. Clinical case
A 14-year-old male patient arrived at the internal medicine department due to facial
asymmetry with size increase of the right side of the face for approximately 5 years,
without any other symptoms. He denies any personal pathological or surgical history,
with a complete vaccination schedule. Physical examination revealed the previously
described facial asymmetry, harmony of the upper and lower extremities, and Tanner
Score according to age. The rest of the examination shows no significant findings.
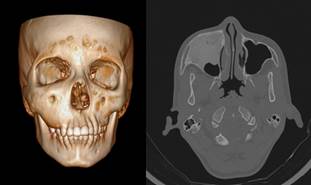
In a tomography of the skull and paranasal sinuses (Figure 1), an expansive sclerotic lesion with ground glass density is evident at the level
of the upper jaw and right zygomatic region, which remodels and reduces the size of
the respective paranasal sinus.
Figure 1
3D skull tomography and axial tomography of the paranasal sinuses with bone window.
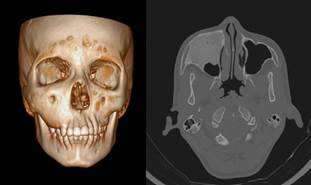
Source: SOLCA Hospital - Guayaquil.
A radiological series is performed on both hands, backbone, lumbosacral, pelvis and
femur with a bone age according to that of the patient, without pathological findings.
In laboratory studies, parathyroid hormone 59.3, LH 4.12, FT4 1.32, TSH 2.93, testosterone
6.12 and vitamin D 28.38 were reported; thus, he received vitamin D3 40 000 IU for
2 weeks and zolendronic acid 4 mg intravenously in a single dose.
An excision of the benign tumor and a Cadwell biopsy of the right jaw was performed.
Its microscopic study confirmed the diagnosis of fibrous bone dysplasia.
He was intervened for a right maxillectomy, mesh placement under 3D planning and reconstruction
with a temporal flap, without complications. The pathology report revealed a homogeneous
whitish-brown mass measuring 7.2 x 5.4 x 4.4 cm and confirmed the previous diagnosis.
Twelve days after the surgical procedure, a new tomographic study of the face (Figure 2) was performed, in which post-surgical inflammatory changes were identified at the
level of the surgical bed that extended to the lateral edge and floor of the orbit,
as well as the right lateral wall of the orbit, nasal cavity and ipsilateral temporal-parietal
region, without evidence of residual lesion and/or recurrence of the tumor.
Figure 2
Axial tomography with contrast 12 days after surgery.

Source: SOLCA Hospital - Guayaquil.
Sixteen days after surgery, the patient was evaluated in the outpatient clinic, showing
improvement of the facial asymmetry, with a favorable condition.
3. Discussion
Fibrous bone dysplasia is a rare pathology with a wide phenotypic and multi-organ
spectrum, whose diagnosis is often challenging in the Internal Medicine field. Also,
this condition can affect a single bone (monostotic, as in this case), or several
(polyostotic). The former is more prevalent in 70-80% of cases [6,7]. There is no data that determines the prevalence of this disease in Ecuador [8].
Extraosseous manifestations might be associated with café-au-lait macules, hyperthyroidism,
acromegaly/gigantism, and abnormal production of testosterone or estrogen, as defined
in McCune-Albright syndrome [9,10]; or coexist with intramuscular myxomas in Mazabraud syndrome [1]. During the physical and complementary examinations of this case, none of these
alterations were evident.
The diagnostic confirmation of the disease is anatomical-pathological, more reliable
for monostotic conditions, since there are several differential diagnoses such as
cancer, simple bone cyst, Paget's disease, ossifying fibroma, and giant cell granuloma
[1,5,11]. Its malignant transformation is very rare in this type of dysplasia (between 0.4
to 4%) and could help determine polyostotic conditions [12].
Surgery is one of the main treatment options considering the site of the condition
and the characteristics of the patient [9]. Various indications for this procedure in craniofacial conditions include compressive
neuropathies (such as the optic nerve), severe malocclusion, bone pain resistant to
analgesic treatment, high risk of recurrence of the deformity and cosmetic purposes
[4,8,13].
Other therapeutic options are bisphosphonates due to their inhibition of bone resorption
and decrease of osteoclast production; however, they did not show improvement in radiological
findings or in the prevention of expansion of bone lesions [14,15]. Despite this, some intravenous formulations, such as zolendronic acid or pamidronate,
have a better therapeutic role compared to the oral route in the treatment of pain
related to bone fibrosis [14,16]. Prior to using antiresorptive drugs, it is important to determine the levels of
kidney function and calcium phosphorus metabolism (including vitamin D and parathyroid
hormone), in case it is necessary to supplement due to deficiencies [3].
Apart from the use of bisphosphonates, another choice includes anti-RANKL antibodies
(denosumab) and anti-IL6, which inhibit bone proliferation and reduce pain symptoms,
respectively, in case bisphosphonates do not have good efficacy or are contraindicated
[15,17].
4. Conclusions
Fibrous bone dysplasia is a benign and rare disease characterized by abnormal growth
of bone tissue, which may be accompanied by dermatological and/or endocrinological
alterations. Early diagnosis allows for more exhaustive studies and more effective
therapy and relief for the patient, highlighting surgical resolution as the first
step.
1. Introducción
La displasia fibrosa ósea es una patología rara, benigna y congénita que afecta el
desarrollo esquelético del cuerpo humano y altera la composición normal del hueso
[1]. Tiene una prevalencia global de 1/100 000 habitantes y engloba el 5 % de los tumores
primarios óseos [2]. A pesar de que su etiología no está clara, se han identificado mutaciones poscigomáticas
del gen GNAS, localizado en el cromosoma 20, que dan lugar a la estimulación de adenilil
ciclasa y posterior sobreproducción de adenosina monofosfato cíclico con proliferación
celular descontrolada e inadecuada diferenciación [1,3]. Su espectro clínico es bastante amplio, lo que suele acompañarse con trastornos
dermatológicos o endocrinológicos. El diagnóstico se realiza a través de la historia
clínica, estudios radiológicos en función del hueso afectado y su investigación histopatológica.
El manejo se enfoca en la observación, el uso farmacológico con bifosfonatos y el
tratamiento quirúrgico [4,5]. Hay muy pocos reportes en la literatura médica nacional sobre esta patología benigna,
por lo que se considera fundamental su divulgación científica en el ámbito médico.
2. Caso clínico
Se trata de un paciente masculino de 14 años que acude a la consulta de medicina interna
por presentar asimetría facial, con aumento de tamaño en la hemicara derecha desde
hace aproximadamente cinco años, sin ninguna otra sintomatología. Niega antecedentes
patológicos personales o quirúrgicos; cuenta con esquema completo de vacunación. En
el examen físico se evidencia la asimetría facial previamente descrita, armonía de
las extremidades superiores e inferiores y escala de Tanner acorde con la edad. El
resto de la exploración no muestra hallazgos evidentes.
En la tomografía de cráneo y senos paranasales (Figura 1), se evidencia una lesión expansiva esclerótica con densidad de vidrio esmerilado
en el maxilar superior y la región cigomática derecha, que remodela y disminuye de
tamaño el seno paranasal respectivo.
Figura 1
Tomografía de cráneo 3D y tomografía axial de senos paranasales con ventana ósea.
Fuente: Hospital SOLCA - Guayaquil.
Se realizó una serie radiológica a en manos, columna dorsal y lumbosacra, pelvis y
fémur con una edad ósea acorde a su edad, sin hallazgos patológicos.
En los estudios de laboratorio, se reportó hormona paratiroidea 59.3, LH 4.2, FT4
1.32, TSH 2.93, testosterona 6.12 y vitamina D 28.38, por lo que recibió vitamina
D3 40000 UI por dos semanas y ácido zolendrónico 4 mg por vía intravenosa en dosis
única.
Se optó por realizar una escisión del tumor benigno y biopsia vía Caldwell en el maxilar
derecho, cuyo estudio microscópico confirmó el diagnóstico de displasia fibrosa ósea.
Fue intervenido quirúrgicamente con maxilectomía derecha, colocación de malla bajo
planificación 3D y reconstrucción con colgajo temporal, sin complicaciones. En el
reporte patológico se evidenció una masa homogénea parda blanquecina de 7.2 x 5.4
x 4.4 cm, con un estudio que confirmó el diagnóstico de displasia fibrosa.
Doce días después del procedimiento quirúrgico, se evaluó con nuevo estudio tomográfico
de cara (Figura 2), en el cual se identificaron cambios inflamatorios posquirúrgicos en el lecho quirúrgico
que se extendían hasta el borde lateral y piso de la órbita, así como a la pared lateral
derecha de la cavidad nasal y región temporoparietal ipsilateral, sin datos de lesión
residual o recidivante del tumor.
Figura 2
Tomografía axial de cara simple con contraste.

Fuente: Hospital SOLCA - Guayaquil.
Después de 16 días de la cirugía, el paciente fue valorado en consulta externa y mostró
mejoría de la asimetría facial, con una evolución favorable.
3. Discusión
La displasia fibrosa ósea es una patología rara con un amplio espectro fenotípico
y multiorgánico, cuyo diagnóstico suele ser desafiante en el campo de la medicina
interna. Esta patología puede afectar a un solo hueso -ser monostótica, como en este
caso-, o a varios de estos (poliostótica). La primera forma es más prevalente en un
70-80 % de los casos [6,7]. No hay datos que determinen la prevalencia de esta enfermedad en Ecuador [8].
Cabe mencionar que pueden asociarse manifestaciones clínicas extraóseas como las máculas
de café con leche, hipertiroidismo, acromegalia/gigantismo y producción anormal de
testosterona o estrógenos, definidas en el síndrome de McCune-Albright [9,10]. También pueden coexistir con mixomas intramusculares en el síndrome de Mazabraud
[1]. En la exploración física y exámenes complementarios del caso, no se evidenció ninguna
de estas alteraciones.
La confirmación diagnóstica de la enfermedad se realiza con la biopsia, y la más razonable
es la de afección monostótica, pues existen varios diagnósticos diferenciales como
el cáncer, el quiste óseo simple, la enfermedad de Paget, el fibroma osificante y
el granuloma de células gigantes [1,5,11]. Su transformación maligna es muy rara en este tipo de displasia (entre el 0.4 y
el 4 %), factor que condiciona a ello su afección polióstica [12].
Uno de los pilares del tratamiento es la cirugía, considerando tanto el sitio de afección
como las características del paciente [9]. Varias indicaciones para este procedimiento en afecciones craneofaciales comprenden
neuropatías compresivas, como el nervio óptico, la mala oclusión severa, el dolor
óseo resistente al tratamiento analgésico, el alto riesgo de recurrencia de la deformidad
y los fines cosméticos [4,8,13].
Otras opciones terapéuticas son los bifosfonatos por su inhibición en la resorción
ósea y disminución de la producción de osteoclastos; sin embargo, esta opción no mostró
mejoría en los hallazgos radiológicos ni en la prevención de la expansión de lesiones
óseas [14,15]. A pesar de ello, algunas formulaciones intravenosas, como el ácido zoledrónico
o el pamidronato, tienen un mejor rol terapéutico en comparación con la vía oral en
el tratamiento del dolor relacionado con la fibrosis ósea [14,16]. Previo a la utilización de los fármacos antirresortivos, es importante determinar
los niveles de función renal y metabolismo fosfocálcico (incluyendo la vitamina D
y la hormona paratiroidea), para considerar la posibilidad de administrar suplementación
en caso que existiese alguna deficiencia [3].
Además del uso de bifosfonatos, otra elección comprende los anticuerpos anti-RANKL
(denosumab) y los anti-IL6, que inhiben la proliferación ósea y disminuyen la sintomatología
del dolor, respectivamente, en caso de que los bifosfonatos no tengan una buena eficacia
o se encuentren contraindicados [15,17].
4. Conclusiones
La displasia fibrosa ósea es una enfermedad benigna e infrecuente que se caracteriza
por el crecimiento anómalo del tejido óseo y que puede acompañarse de alteraciones
dermatológicas o endocrinológicas. La sospecha diagnóstica brinda estudios más exhaustivos
en época temprana, y estos determinarán una terapéutica más eficaz y alivio del paciente.
Se destaca como primer escalón la resolución quirúrgica.